

If your weight is causing health problems and nothing you’ve tried has worked, it may be time to look into weight loss surgery.
Dr. Kimberley Steele Johns Hopkins Center for Bariatric Surgery
With two out of three over-weight and one in three obese, over 200,000 Americans annually choose some form of weight loss surgery to loose enough weight to improve their health. But is it for you? And which one of the procedures would you choose? My video interview with Dr. Kimberley Steele explains the procedure.
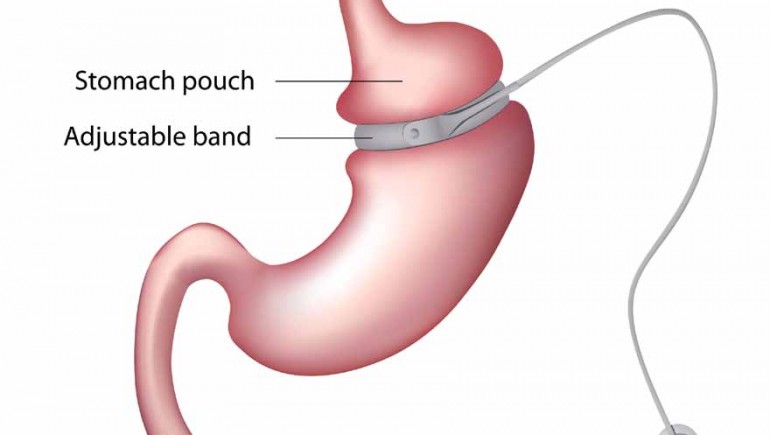
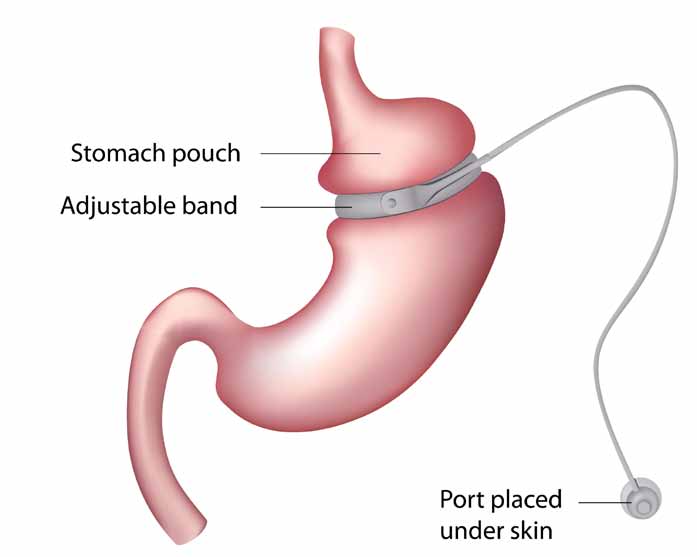
Adjustable Gastric Band (Lap-Band)
Dr. Mache Seibel: Who’s a good candidate to have surgery to lose weight?
Dr. Kimberley Steele: I think that we have to still follow the NIH Guidelines, which state that the patient who has a BMI > 40 without any medical complications; or, a patient with a BMI > 35 with multiple medical problems.
Dr. Seibel: So, a BMI is a body mass index and that’s an indicator of weight that uses your height and your weight together in a mathematical formula. So, it’s people who are really pretty darn overweight and basically if you need a seat belt extender in the airplane, you’ve probably got a BMI of 40. If your BMI is 35, you’re not quite that big, but if you have that plus some other illnesses, you’re a candidate.
Dr. Steele: Yes. Now, the FDA did in February of 2011 approve the Lap-Band product for a BMI of 30 if the patient has severe medical problems.
Dr. Seibel: Tell us what a Lap-Band is.
Dr. Steele: A Lap-Band is a plastic device that looks like a belt that goes around the top part of the stomach. It’s attached to a catheter and the catheter is attached to a port placed just under the skin in your fat, so you can’t see it. You can feel it though. You come in and the doctor adjusts it by putting saline solution into that port, which tightens the band. The tighter it is, the more restrictive it is. And the idea is that it’s restriction only. It is the least invasive of the procedures that we offer, and basically, it decreases the amount that you can eat at any one time. However, the patient has to realize it does not de-crease their hunger. And so, a patient who eats ice cream, milk shakes, “M&Ms that “melt in your mouth, not in your hands,” potato chips, sugary beverages is not going to drop the weight because those foods slither through the band.
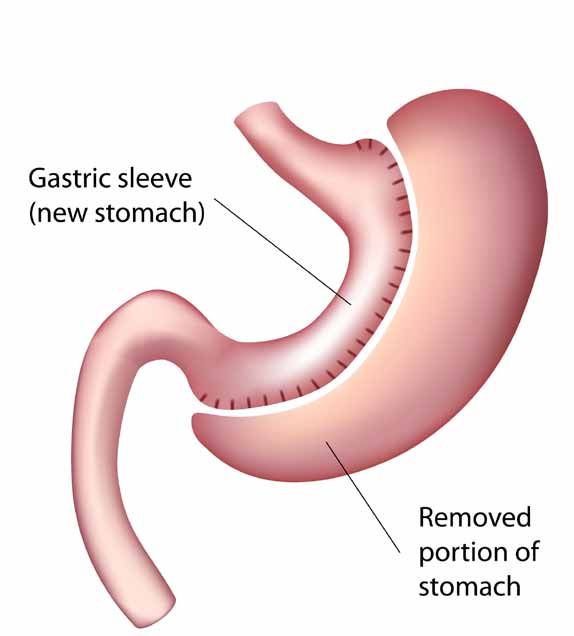
Vertical Sleeve Gastrectomy
Dr. Seibel: So, you can literally eat your way through it by eating caloric liquids and candies, but if you eat solid foods, it will slow you down.
Dr. Steele: Slow you down. Right. The other thing is that patients have to be aware if they’re grazers – and what we mean by “grazers” is they pick all day long in small amounts – this too will not lead to a very good result with the Lap-Band. Dr. Seibel: In addition to using a band to restrict the entrance to the stomach, you can also remove part of the stomach. Tell me about that. Dr. Steele: That’s called the laparoscopic vertical sleeve gastrectomy.
The idea is that you take a stomach that’s about the size of a football and you make it about the size of a banana; so it only holds about 100 cc’s or about 4.3 ounces. It’s also fairly restrictive. Some people say that it also gives you somewhat less hunger because you are removing some of the ghrelin component.
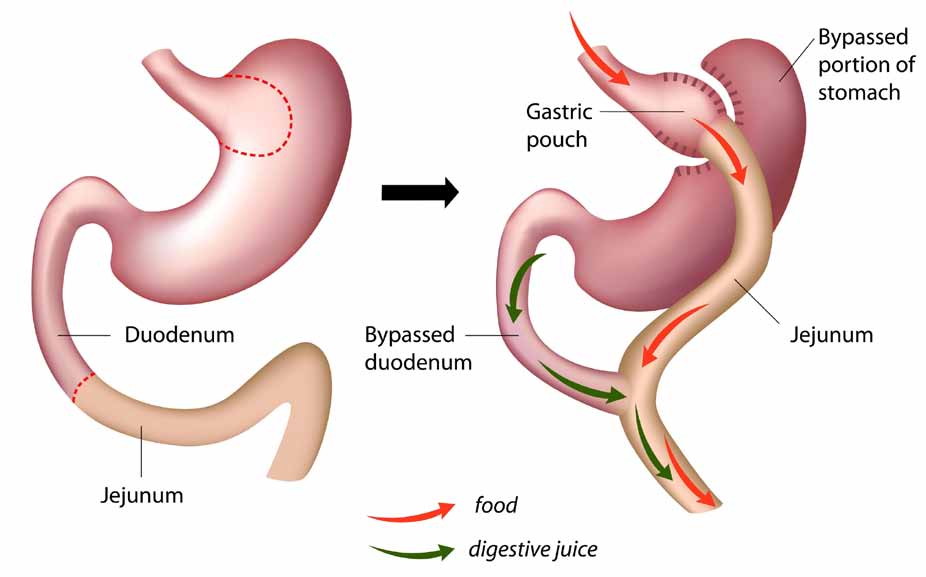
Rou-en-Y Gastric Bypass
Dr. Seibel: That’s a stomach hormone that makes you feel hungry.
Dr. Steele: Correct. The stomach releases ghrelin. Some studies suggest the vertical sleeve decreases the ghrelin and that decreases your hunger. We remove at least three quarters of the stomach. The patient has to realize once we remove it, we can’t give it back and they’re left with a very tiny stomach and that restricts the amount that they can eat at any one time. Again, very similar to the band, if you eat liquid foods or if you graze all day long, it’s not going to work. You have to understand that you’ve got to follow a specific diet and be compliant to have good success. But generally, we see very nice results. There’s 5-year data out now that suggest patients lose at least 40% of their excess body weight with less complications.
Right after surgery, we see patients whose diabetes and high blood pressure goes away. Some of them leave the hospital off their medications immediately.
Dr. Seibel: Okay. There is also other more involved surgery.
Dr. Steele: Correct. The Laparoscopic Roux-en-Y Gastric Bypass or the Open Roux-en-Y Gastric Bypass is both a restrictive and a malabsorptive procedure. This procedure is restrictive because we actually transect the stomach and make a very tiny pouch about the size of an egg, and we also bypass a portion of the stomach to allow malabsorption. Very minimal malabsorption, but enough that the two parts of this process – both restrictive and malabsorptive — help the patient lose weight. And we’re able to tell patients that at least 80% who under-go this procedure will lose anywhere from 50% to 75% of their estimated excess body weight.
Dr. Seibel: That’s a lot. Fifty to 75% of the overweight amount will go away. So this operation disconnects the stomach from the tube that comes down to it, the esophagus, and you leave it in. You also make a cut in the small intestine about a 100 cm. (about 3 feet away), and then you connect those two parts — you just leave that other part in there. It’s all living and healthy, but it’s not get-ting any food.
Dr. Steele: Correct. And that part that is not getting any food is the part that carries the bile from the liver and the pancreatic enzymes that help digest the food. That’s what creates more weight loss for the patient and why we see nice results. The other advantage of the Roux-en-Y Gastric Bypass is the fact that you can heal medical problems so quickly.
Dr. Seibel: And the reason that you do the surgery is not because they’re fat…
Dr. Steele: I’m very clear with the patients that I operate on that this is not cosmetic. It is work and a lifetime commitment. And as long as they are compliant they should sail through it. I really do believe that patients that do what they’re supposed to do, do great. And the ones that are non-compliant (and they will admit to it) are the ones that we generally don’t see the success or they have problems, and those problems can be very significant. When they follow what they’re supposed to do, we’re seeing really nice results. I think the big thing is to realize is this is major surgery and there’s no snapping of the finger or waving a magic wand. They have to commit to it and do the work to have the success; and with that, they will be successful.
